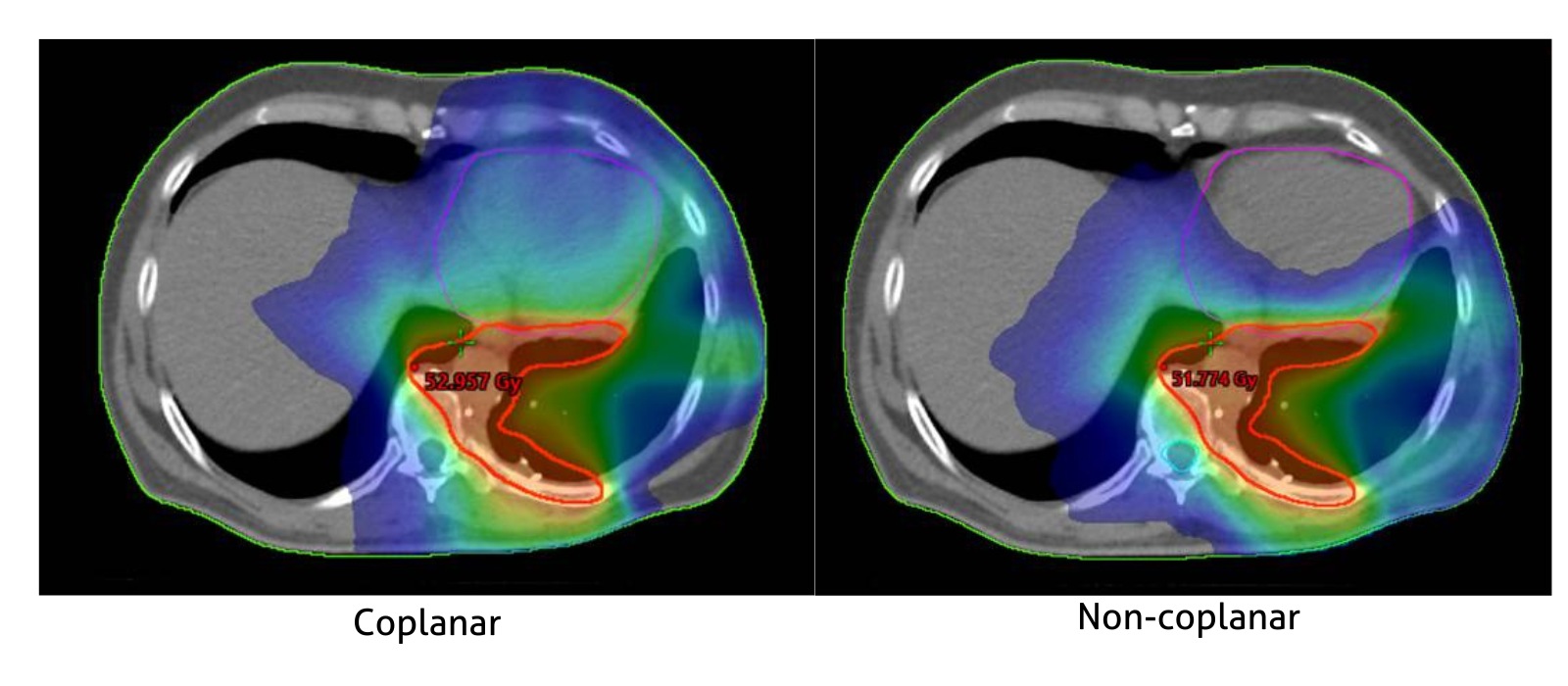
Achieve Lower Organ at Risk Dose With Non-Coplanar Treatments and Surface Guided Clearance Mapping
Images courtesy of Dipl Ing K Hierholz,
Klinikum Darmstadt
Recent studies show non-coplanar treatments can deliver clinically relevant improvements to treatment plans1, specifically in liver cancer2, lung cancer 3-10, breast cancer 11-14, head and neck cancer15-21, lymphoma22,23, and prostate cancer24. Traditionally, non-coplanar treatments require extra planning and machine time, both for dry runs and treatments. Additionally, some non-coplanar plans are not deliverable, which can lead to complicated re-planning and repeat quality assurance work, leading to delays in patient treatment and increased costs.
This becomes even more important in reirradiation cases, where finding feasible beam paths is more challenging due to prior dose limits and anatomical constraints, something traditional planning tools often struggle with.
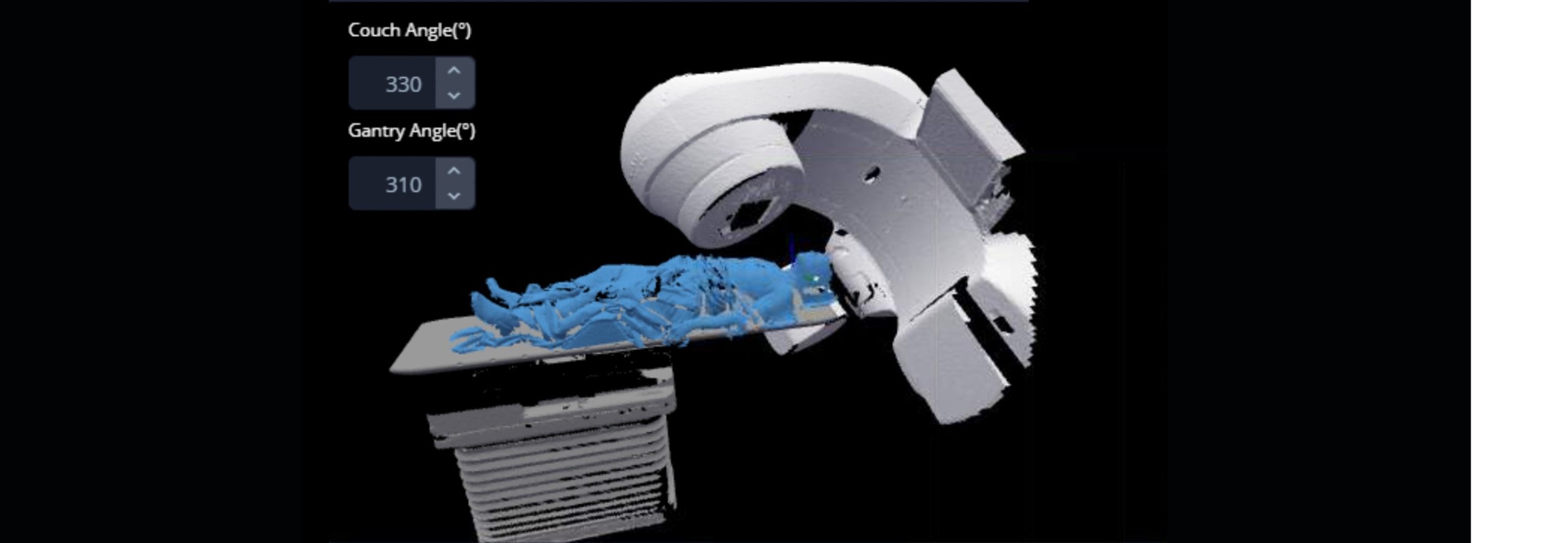
MapRT is designed to help overcome the practical challenges of non-coplanar treatments.
Users can select the optimal safe beams or arcs prior to planning, check for safe beam transitions and understand the maximum safe couch and gantry angles that are possible for each patient in their treatment position25-27.
Recent Research on Non-Coplanar Treatments:
All studies quoted here are VMAT coplanar vs VMAT non-coplanar unless stated otherwise.
The additional degrees of freedom are shown to increase the therapeutic ratio, either through dose escalation to the target or dose reduction to functionally important organs at risk, by multiple research groups. Although significant work is still needed to translate these new non-coplanar radiotherapy techniques into the clinic, clinical implementation should be prioritized.¹
Nine [lung cancer] studies were included and evaluated in the meta-analysis [including VMAT and other techniques], and treatment plans were designed with both coplanar beam arrangements CBA and non-coplanar beam arrangements (NCBA). After combining multicenter results, NCBA plans have significant advantages in reducing V20 of the whole lung and max dose of spinal cord [versus CBA].5
Non-coplanar VMAT proposed in this study showed more favorable plan quality than the coplanar VMAT plans for lung SABR with tumors located close to the heart.6
Static couch non-coplanar optimization yielded maximum dose reductions to OARs while maintaining target conformity for lung SBRT.7
For middle and lower lung tumors…a significant reduction in equivalent uniform dose, V30, V40 and V50 is observed for the heart when either non-coplanar fields or IMRT is used. IMRT also reduces the lung NTCP, V5, V13, V20 and V30 values and esophagus NTCP.8
Doses to the heart and ipsilateral lung were significantly lower with non-coplanar VMAT compared to both coplanar VMAT and 3D-CRT. Non-coplanar VMAT reduced doses to both the contralateral breast and lung compared to coplanar VMAT and achieved levels similar to 3D-CRT for the contralateral breast and moderately higher doses for the contralateral lung. Delivery of high doses (>30 Gy) to the contralateral side was completely avoided with non-coplanar VMAT, contrary to the results for coplanar VMAT and 3D-CRT.11
[In left-sided breast cancer] Compared to coplanar VMAT, non-coplanar VMAT provides improved conformity and homogeneity of whole PTV, better dose sparing of the heart, bilateral lungs, left anterior descending coronary artery (LAD), and right breast for locoregional radiotherapy of left-sided breast cancer with IMN, potentially reducing the risk of normal tissue damage.13
[In this study of bilateral breast cancer cases] VMAT plans with non-coplanar beam arrangements had significant dosimetric advantages in terms of sparing of critical organs, that is Dmean of heart doses with almost equivalent lung doses and equally good target coverage.14
[For patients in our study of] postoperative stereotactic body radiotherapy (SBRT) in case of high-risk margins for pT1-T2/N0 oropharyngeal and oral cavity tumors … VMAT coplanar + non-coplanar had better dosimetric outcomes than VMAT coplanar and has become the standard technique for patients treated … in our institution. Acute toxicity appears acceptable.15
For the first 15 patients on a prospective phase II clinical trial exploring the safety, feasibility, and efficacy of the [non-coplanar] technique for recurrent head and neck cancer treatment. … statistically significant increases in dose conformity and mean PTV and GTV doses. With a median follow-up of 12 months … patient-reported QOL metrics were favorable. … treatment delivery was feasible, safe, and well-tolerated by patients. 16
Twenty-five previously treated patients of HNC underwent re-planning to improve the dose distributions with either coplanar VMAT technique … or noncoplanar … VMAT plans. [Non-coplanar] VMAT plans allowed to decrease the dose-volume-metrics for relevant OAR and results are reliable from a dosimetric standpoint.18
Automated non-coplanar VMAT achieved superior one-year local control compared to the historical local control rate without higher grade ≥ 3 toxicity. This represents one of the highest local control rates reported in a prospective trial of head and neck re-irradiation and a new approach to head and neck SBRT.21
[In treatment of nasopharyngeal tumours] VMAT using optimized non-coplanar irradiation trajectories reduced the mean and maximum doses in organs at risk compared to coplanar VMAT plans by 19% on average while the target coverage remains constant.19
VMAT provided significantly better target coverage, in terms of V100% (Volume encompassed by the isodose 100%), than IMRT, in particular when nc-VMAT was used. In general, organ at risk sparing is similar with the three approaches, although nc-VMAT can allow a statistically significant reduction of dose to contralateral parotid gland and cochlea.20
Overall there was a clear tendency towards higher plan quality with non-coplanar configurations. B-VMAT resulted in reduced low-dose spread in lungs and left breast. Non-coplanar beam configurations were favorable for young female mediastinal lymphoma patients, with patient-specific and plan-parameter-dependent dosimetric advantages.22
Non-coplanar IMRT had better PTV coverage and OARs sparing, except for being larger in V5 to breast and lung. In IMRT for young female patients with mediastinal lymphoma, using of non-coplanar IMRT significantly reduces the radiation dose to the breasts and lungs compared with coplanar IMRT, and consequently reduces the risk of breast second cancer and pulmonary toxicity. Besides young female patients, non-coplanar IMRT can also benefit other mediastinal lymphoma patients.23
“The proposed two-beam non-coplanar class solution to complement coplanar dual-arc VMAT resulted in substantial plan quality improvements for OARs (especially rectum) and reduced irradiated patient volumes with minor increases in treatment delivery times”.24
Hear from users on their clinical experiences:
“A simple thing like adding one non-coplanar arc can make a dramatic difference in the plan quality, can significantly reduce the dose to OARs and have a meaningful impact on the patient’s quality of life.”
Kiran Kumar, MD, University of Texas Southwestern
“We are thinking that [non‑coplanar] treatment will be new standard next year for head and neck.”
Mathieu Gonod, Medical Physicist, Centre G.F. Leclerc, France
MapRT is protected under various granted and pending patents, including US Issued Patent 10,549,116 (Filed January 3rd, 2016)
Get in touch
Ready to take the next step?
Vision RT’s family of SGRT solutions guide radiation therapy for better patient care at every step: Sim, Planning, Treatment and Dose. Whether you’re looking for a quote, a product demo (virtual or in-person) or just more information, please get in touch.