Bilder zur Verfügung gestellt von
Dipl.-Ing. K. Hierholz, Klinikum Darmstadt
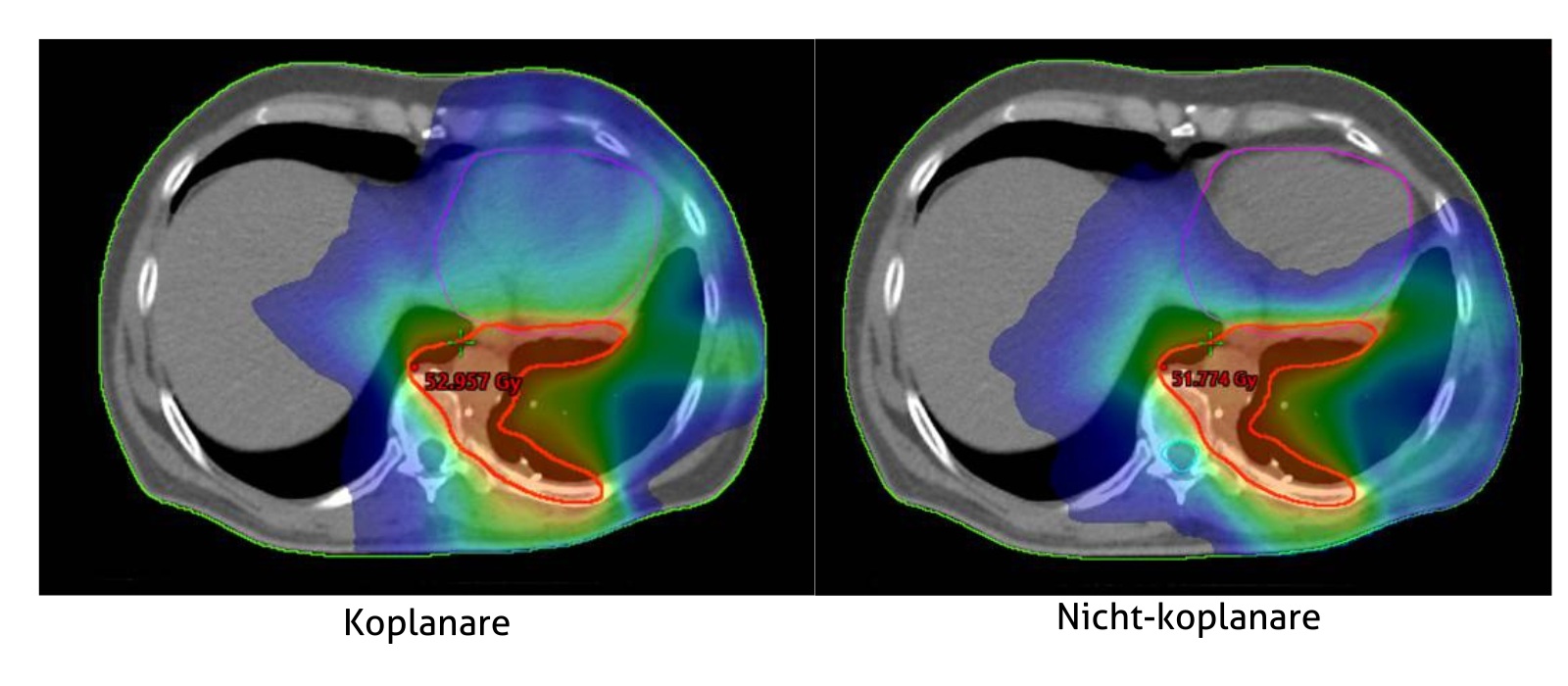
Aktuelle Studien zeigen, dass nicht-koplanare Behandlungen klinisch relevante Verbesserungen der Behandlungspläne1, bewirken können, insbesondere bei Lungenkrebs 2,3,4,5 Brustkrebs6,7,8,9,, Kopf- und Halskrebs 10,11,12,13,14, Lymphome15, 16, und hochgradiges Gliom 17. Traditionell erfordern nicht-koplanare Behandlungen zusätzliche Planungs- und Maschinenzeit, sowohl für Probeläufe als auch für Behandlungen. Darüber hinaus sind einige nicht koplanare Pläne nicht bestrahlbar, was zu komplizierten Neuplanungen und wiederholten Qualitätssicherungsarbeiten führen kann, welches zu Verzögerungen bei der Patientenbehandlung und höheren Kosten führt.
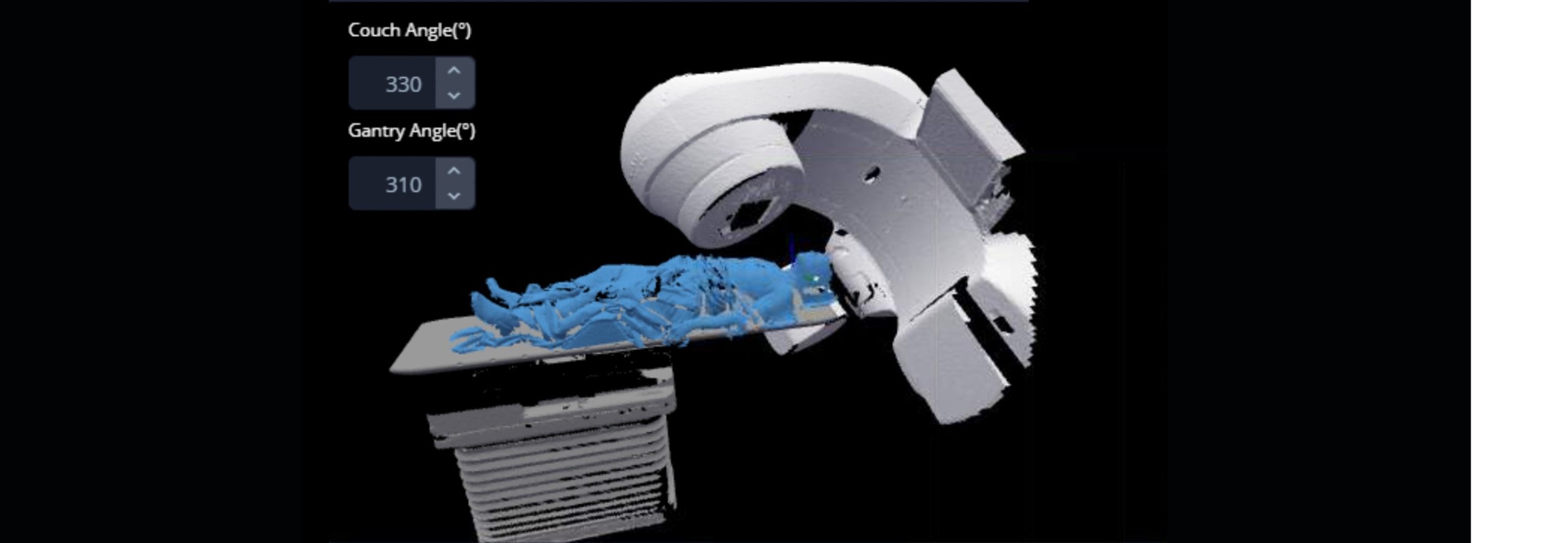
MapRT soll dazu beitragen, die praktischen Herausforderungen nicht koplanarer Behandlungen zu meistern: Überprüfung auf nutzbare Tisch- und Gantrywinkel während der Planung, Kartierung sicherer Strahlübergänge und Anzeige der maximal sicheren Tisch- und Gantrywinkel, die für jeden Patienten in seiner Behandlungsposition möglich sind.
Aktuelle Forschungsergebnisse zu nicht-koplanaren Behandlungen:
MapRT ist durch verschiedene erteilte und angemeldete Patente geschützt, einschließlich des erteilten US-Patents 10,549,116 (eingereicht am 3. Januar 2016)
Nehmen Sie Kontakt auf
Bei Vision RT legen wir großen Wert auf unsere Reaktionsfähigkeit und unseren Kundenservice.
Ob Sie ein Angebot, eine Demo (virtuell oder persönlich) oder einfach mehr Informationen suchen, nehmen Sie bitte Kontakt mit uns auf bezüglich AlignRT oder einem unserer anderen Produkte: